신경통 근위축증 환자에서 국소 및 전신 스테로이드 병용 치료: 증례 보고
The Successful Treatment of Combined Local and Systemic Steroids in a Patient with Brachial Plexus Neuritis: A Case report
Article information
Trans Abstract
Brachial plexus neuritis (BPN), also known as Parsonage-Turner syndrome, is an uncommon neurological disorder that can manifest with acute extreme upper arm pain followed by patchy muscle paralysis. There is no evidence supporting any recommended treatments for BPN from randomized trials. Non-randomized studies have supported the effectiveness of early administration of high-dose oral corticosteroids during the painful phase. We present a case of a 41-year-old-female with a history of acute left lateral shoulder pain and shoulder girdle weakness who was diagnosed with acute BPN. To reduce the risk of complications arising from high-dose oral steroid administration, we used an ultrasound-guided brachial plexus blockade combined with low-dose oral steroids. The combined treatment approach successfully restored shoulder function and effectively alleviated pain while avoiding complications associated with systemic steroid administration.
Introduction
Brachial plexus neuritis (BPN) is a rare peripheral nervous disorder characterized by acute attacks of neuralgia and patchy paresis on upper extremities followed by weakness and atrophy. The pathophysiologic mechanism underlying BPN is presumed to involve localized inflammatory or immune processes affecting the brachial plexus [2]. High-dose oral corticosteroid therapy is the conventional treatment strategy for ameliorating the acute painful phase of BPN [1,3]. Among patients who receive high-dose oral steroid therapy, 20% to 30% experience systemic side effects, including gastrointestinal complaints and mood swings [1,4]. As for other treatments, pain medications (including opioids and gabapentin) or physical therapy (including transcutaneous electrical nerve stimulation) can be applied in the acute and delayed phases [3].
To reduce localized brachial plexus inflammation and to minimize the systemic side effects of steroids, we performed three ultrasound-guided brachial plexus blockades combined with low-dose oral steroid administration. This treatment strategy achieved full restoration of shoulder-girdle function and elimination of residual shoulder pain within 3 months after onset.
Case report
Two weeks after recovering from a common cold, a 41-year-old, right-handed woman experienced sharp and acute pain in her left shoulder and lateral upper arm, followed by a marked loss of left shoulder mobility. The symptoms were so severe that the patient had difficulty completing daily activities. She visited our hospital 2 weeks after the onset of pain. She rated her pain as 7 out of 10 on a numeric rating scale (NRS) ranging from “no pain" (0) to the "most severe pain imaginable” (10). She described a tingling sensation and a dull ache affecting the left shoulder and lateral upper arm. She denied a previous history of neck pain or radiating pain before this event. There was no history of hereditary or metabolic disease. Pain medications, such as opioids, provided no significant pain relief.
Upon physical examination, the patient had prominent left shoulder girdle muscle weakness without atrophy. Shoulder flexion and abduction exhibited Medical Research Council (MRC) power gradings of 2/5, and elbow flexion was graded as 4/5. Her muscle power was normal in the left wrist and hand, as well as the entire right upper extremityLight touch and pin-prick test results were unremarkable. Passive shoulder movement achieved the full range of motion in all directions. Spurling’s test results, which assesses radicular pain, was unremarkable. The Neer and Hawkins–Kennedy tests for identifying rotator cuff pathology were negative.
Her white blood cell count, C-reactive protein and rheumatoid factor results were within normal limits. HbA1c was 5.6. The motor and sensory nerve conduction studyresults were also within normal limits (Table 1). However, electromyography revealed signs of denervation of the left infraspinatus, deltoid, biceps bracii, and left cervical paraspinalis muscles (Table 2). Cervical magnetic resonance imaging (MRI) showed a herniated disc at the C4–5 level with mild protrusion in the left foraminal zone and bulging discs at the C5–6 and C6–7 levels without neural foraminal stenosis or severe cervical root compression.

Motor and Sensory Nerve Conduction Study Results
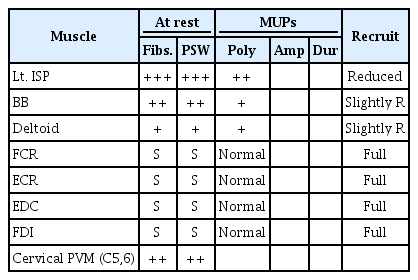
Needle Electromyography
As a differential diagnosis, cervical radiculopathy was deemed unlikely since the patient presented with sudden pain and severe weakness of the shoulder girdle in a short period without any history of trauma or neck pain. Additionally, the physical examination findings did not support this diagnosis, nor did the mild herniated disc at C5–6—it was not a lesion that could cause severe acute paralysis. Rotator cuff disease was ruled out because of intact range of motion, along with the negative Neer and Hawkins–Kennedy tests and the intact rotator cuff tendon revealed by ultrasound examination. We conducted a brachial plexus MRI with contrast enhancement after suspecting a diagnosis of acute idiopathic BPN. The MRI findings were as follows: 1) mild swelling at the post-ganglionic level of the C5 nerve, 2) swelling and high signal intensity in the left trunks, divisions and the lateral cord and 3) mild T2 high signal intensity at the left supraspinatus and infraspinatus muscles, suggesting denervation changes related to the suprascapular nerve (Fig. 1A, B, and C). Based on the clinical manifestations and radiologic findings, an initial working diagnosis of idopathic BPN was made.

Brachial plexus MRI with contrast enhancement for a patient with BPN. A) T2 water-excited sagittal image: mild nodular swelling observed in the post-ganglionic level of the C5 nerve root; B) T2 water-excited coronal image:s swelling and high signal intensity observed in the left trunks, divisions, and lateral cord; C) T2 water-excited sagittal image: mild–high signal intensity in the left supraspinatus (SSP) and infraspinatus (ISP), suggesting a denervation change related to the suprascapular nerve.
Considering the acute painful phase of the idopathic BPN, we initiated oral steroid therapy (30 mg prednisolone for the first 5 days, tapered to 20 mg for 3 days, 10 mg for 1 week, and ending with 5 mg as a maintenance dose). The timing of oral prednisone cessation was to be guided by the patient’s symptoms. The patient was scheduled for ultrasound-guided brachial plexus blockades to facilitate an oral steroid dosage reduction and provide direct control of local inflammation.
To evaluate the outcomes of the treatment, we assessed the MRC power grades for the three muscle pairs (shoulder flexors, abductors, and elbow flexors), and pain was reassessed using the NRS (Fig. 2). An experienced physician administered an initial injection (dexamethasone 5 mg + lidocaine 25mg) to the C5 brachial root 2 weeks after the onset of symptoms. Two weeks after the first injection, the power in the shoulder flexors and abductors improved from MRC grade 2 to grade 3, and the NRS dropped from 7 to 3. Since the patient was experiencing pain relief and muscle strength improvement, along with greater overall satisfaction, the second injection was administered to the same site with the same drug concentration. Two weeks after the second injection, the pain score went down further, from 3 to 2, and the MRC grades for shoulder abduction and flexion improved from 3 to 4. Since the upper arm pain and shoulder weakness persisted somewhat, a third injection (triamcinolone 20mg + lidocaine 25mg) was finally administered at the trunk level (Fig. 3), and we stopped the oral prednisolone. During the period taking oral steroids, she had no side effects such as nausea, gastrointestinal discomfort, weight gain. Three months after the onset of symptoms, the patient's muscle power was fully restored, and her pain had subsided. Monitoring for side effects was conducted after each injection; however, no side effects of the intervention such as dyspnea, hoarseness, paralysis and local infection, or bleeding were observed. She reported no functional limitations in the performance of daily activities and returned to work.

The outcome of treatement : The graph shows the changes in the shoulder flexors, abductors, and elbow flexors of medical research council (MRC) grades and the numeric rating scale (NRS) for pain following each steroid injection.

Ultrasound-guided injection to left brachial plexus at the trunk level with 20mg triamcinolone acetonide and lidocaine 25mg. A) Before the injection; B) During injection. SCM: sternocleidomastoid, AS: anterior scalene, MS: middle scalene.
Discussion
Although the precise pathophysiology of BPN remains unclear, the condition is assumed to have unique or multiple focal inflammatory, immunologic triggers [2,3]. From the pathological perspective, the effectiveness of anti-inflammatory and immunomodulatory drugs, including high-dose oral steroids or intravenous immunoglobulin therapy, has been reported [1,5]. These drugs are administered to reduce the fibrous, stenotic changes of some fascicular hourglass-like constrictions and eventually prevent axonal damage [3].
Van Eijk et al. [1] suggested a regimen “60 mg/day (prednisolone) in the first week, tapered by 10 mg every day during the next 5 days, ending with 5 mg on day 13” for acute-onset BPN (< 1 month) patients.After one year, this regimen provided higher recovery rates than management strategies that omitted corticosteroid therapy (56% vs. 11%) [1]. However, about 20% to 30% of patients are reported to experience systemic side effects, including mood swings and gastrointestinal complaints, due to oral corticosteroid therapy [1,4]. In addition, The short-term use of oral prednisone decreases glucose tolerance in a dose-dependent manner, and more than 6 days of high-dose prednisone (>60mg) raises the possibility of hypothalamic–pituitary–adrenal axis suppression even among healthy adults [6].
If attacks of BPN are presumed to be pathologically immune-mediated, we considered localized immune control through steroid injections. Although no clinical studies on this technique have been reported, one report suggests that local anesthetic and steroids can be used as excellent adjuncts to other treatments [7]. The intervention is helpful for pain relief while oral steroids are being titrated to an effective level [7]. In one case report, an 83-year-old man with IBPN was treated with an interscalene brachial plexus block consisting of bupivacaine and dexamethasone [8]. This approach is not without risks, since the procedure itself can result in some complications, including post-interventional pain, ipsilateral hemidiaphragmatic paresis, Horner’s syndrome, and hoarseness [9]. However, the ultrasound-guided approach used by an experienced practitioner would improve the quality of the injection because the approach allows the dynamic visualization of the relevant anatomical structures and needle [9].
In this case, the rationale behind the initial approach to the C5 brachial root was as follows: 1) there was motor paralysis in the C5 myotome and pain in the lateral shoulder area corresponding to the C5 dermatome, 2) the supraspinatus and infraspinatus showed denervation changes on a brachial MRI, and these muscles are innervated by the nerves above the brachial trunk level, and 3) brachial plexus MRI with contrast enhancement also showed a high signal intensity in the post-ganglionic C5 root with mild swelling. The third injection to the brachial plexus in the trunk was finally applied to control the local inflammation shown in the brachial plexus MRI and to prevent progressing axonal damage. These outcomes were desirable in treating our patient.
There are some limitations to consider in association with this report. First, from a case report, we cannot decipher whether the treatment strategy described herein is superior to conventional oral steroid therapy in terms of effecting pain reduction and functional recovery. Further investigations of the efficacy of ultrasound-guided brachial plexus blockades and into the development of a standardized treatment regimen should be undertaken.
In conclusion, althougth, the precise pathophysiology of BPN is unknown, it is thought to be associated with a localized inflammatory immune attack. Additionally, conventional high-dose oral steroid therapy is associated with systemic side effect risk. In our case, the combination of ultrasound-guided steroid injections with low-dose oral steroid therapy successfully relieved pain while avoiding complications associated with systemic steroid administration.Therefore, this approach may be an alternative treatment method to the patients with IBPN who had a risk of high-dose oral steroid side effect.